
All articles
Is Long-Term GLP-1 Use Safe? What 10-Year Data Suggests
Reading time:
10 min

Weight loss

Get expert guidance and a personalized care plan designed around you.
Gastrointestinal Side Effects Over Time
Nausea, vomiting, diarrhea, and constipation are the most common side effects of GLP-1 therapy. These symptoms are usually most intense during the first few weeks of treatment or after dose increases. The important question is whether these side effects persist or worsen with long term use.
Most studies show that gastrointestinal symptoms decrease over time. In the STEP trials, nausea was most common in the first 20 weeks of treatment and declined significantly after that. By one year, most people reported mild or no gastrointestinal symptoms. Discontinuation rates due to side effects were highest in the first few months and dropped sharply after the titration phase.
Some people do experience ongoing digestive changes, such as slower gastric emptying or occasional constipation. These effects are manageable with dietary adjustments, hydration, and fiber intake. Serious complications such as gastroparesis or bowel obstruction are rare and usually occur in people with pre-existing gastrointestinal conditions.
Long term use does not appear to damage the digestive system or cause progressive worsening of symptoms. For most people, side effects stabilize or improve after the first few months.
Pancreatic Safety and Pancreatitis Risk
Pancreatitis has been reported in some people taking GLP-1 medications, though it is rare. Early concerns about pancreatic inflammation and potential links to pancreatic cancer have been studied extensively. Long term data provides clarity on these risks.
Large meta-analyses and cardiovascular outcome trials have not found an increased risk of pancreatitis with GLP-1 use compared with placebo. The rate of pancreatitis in GLP-1 trials is similar to the background rate in people with obesity or diabetes. People with a history of pancreatitis are often advised to avoid GLP-1 medications, but those without prior risk factors do not appear to be at increased risk with long term use.
Concerns about pancreatic cancer have also been addressed. Long term studies have not found higher rates of pancreatic cancer among GLP-1 users. Ongoing surveillance continues to monitor this, but current data is reassuring.
Gallbladder and Kidney Safety
Gallbladder issues, including gallstones and cholecystitis, occur more frequently in people losing weight rapidly. This is true regardless of whether weight loss happens through diet, surgery, or medication. GLP-1 medications are associated with a modest increase in gallbladder events, likely due to rapid weight loss rather than direct effects on the gallbladder.
Long term data from trials such as STEP and SUSTAIN show that gallbladder events are most common in the first year of treatment when weight loss is most rapid. After that, rates stabilize. People with a history of gallstones may be at higher risk, but most people tolerate GLP-1 therapy without gallbladder complications.
Kidney function has also been studied carefully. Early concerns that GLP-1 medications might worsen kidney function have not been supported by long term data. In fact, several studies suggest GLP-1s may protect kidney function in people with diabetes. The FLOW trial, which studied semaglutide in people with diabetes and chronic kidney disease, found that semaglutide reduced the risk of kidney disease progression and kidney-related death.
Bone Health and Muscle Preservation
Weight loss, especially rapid weight loss, can lead to loss of lean muscle mass and changes in bone density. This has raised questions about whether long term GLP-1 use might harm bone health or accelerate muscle loss.
Studies show that people on GLP-1 medications do lose some lean mass along with fat, similar to what happens with any form of calorie restriction. However, the proportion of muscle loss is not greater than what occurs with diet alone. Resistance training and adequate protein intake help preserve muscle during GLP-1 treatment.
Bone density studies in people using GLP-1 medications for one to two years have not found clinically significant bone loss. Some studies suggest GLP-1s may even have neutral or protective effects on bone health. Long term data beyond five years is still limited, but current evidence does not suggest major bone health concerns.
Metabolic Benefits That Persist Over Time
One of the most important findings from long term studies is that metabolic improvements continue as long as people remain on GLP-1 therapy. Weight loss stabilizes after 12 to 18 months, but insulin sensitivity, blood sugar control, blood pressure, and lipid levels remain improved.
The STEP trials found that people who stayed on semaglutide for two years maintained their weight loss and continued to show improvements in HbA1c, fasting glucose, triglycerides, and inflammatory markers. People who stopped the medication regained weight and saw metabolic markers return toward baseline, which suggests that GLP-1 therapy provides ongoing benefit rather than a one-time reset.
Long term liraglutide studies show similar patterns. People who remain on treatment for five years maintain better glycemic control, lower body weight, and reduced cardiovascular risk compared with those who stop. These findings support the idea that GLP-1 medications work best as long term therapies rather than short term interventions.
What Happens When People Stop GLP-1 Therapy
Stopping GLP-1 therapy usually leads to weight regain and reversal of metabolic improvements. This is not unique to GLP-1 medications. It reflects the underlying biology of obesity and metabolic disease. When the medication is removed, appetite signals return, metabolism slows, and the body moves back toward its previous set point.
The STEP 4 trial specifically studied what happens when people stop semaglutide after 20 weeks. Those who discontinued the medication regained most of their lost weight within a year. Those who continued on semaglutide maintained their weight loss and metabolic benefits.
This does not mean GLP-1 therapy is ineffective. It means that obesity is a chronic condition that requires ongoing management. Long term use is often necessary to maintain results, similar to how blood pressure or cholesterol medications work.
Real World Data Beyond Clinical Trials
Clinical trials provide controlled environments with strict monitoring, but real world data captures how GLP-1 medications perform in everyday use. Several large studies using electronic health records and insurance claims data have tracked people using GLP-1 medications for five years or more.
These studies confirm the safety profile seen in trials. Serious adverse events are rare. Most people tolerate the medications well. Cardiovascular benefits persist. Cancer rates remain similar to the general population. Real world data also shows that adherence is a challenge. Many people stop treatment within the first year due to cost, side effects, or lack of support. Those who continue long term see the greatest benefits.
What Researchers Are Still Monitoring
While the long term data is reassuring, researchers continue to track several areas. These include very long term effects beyond ten years, outcomes in younger populations who may use GLP-1s for decades, effects on bone health in older adults, and rare side effects that may only appear with widespread use over time.
Post-marketing surveillance systems track adverse events reported by patients and providers. Registries follow people using GLP-1 medications in real world settings. Ongoing trials continue to study cardiovascular, metabolic, and longevity outcomes.
So far, the safety signals remain strong. GLP-1 medications are among the most studied weight loss therapies available.
Who May Benefit Most From Long Term Use
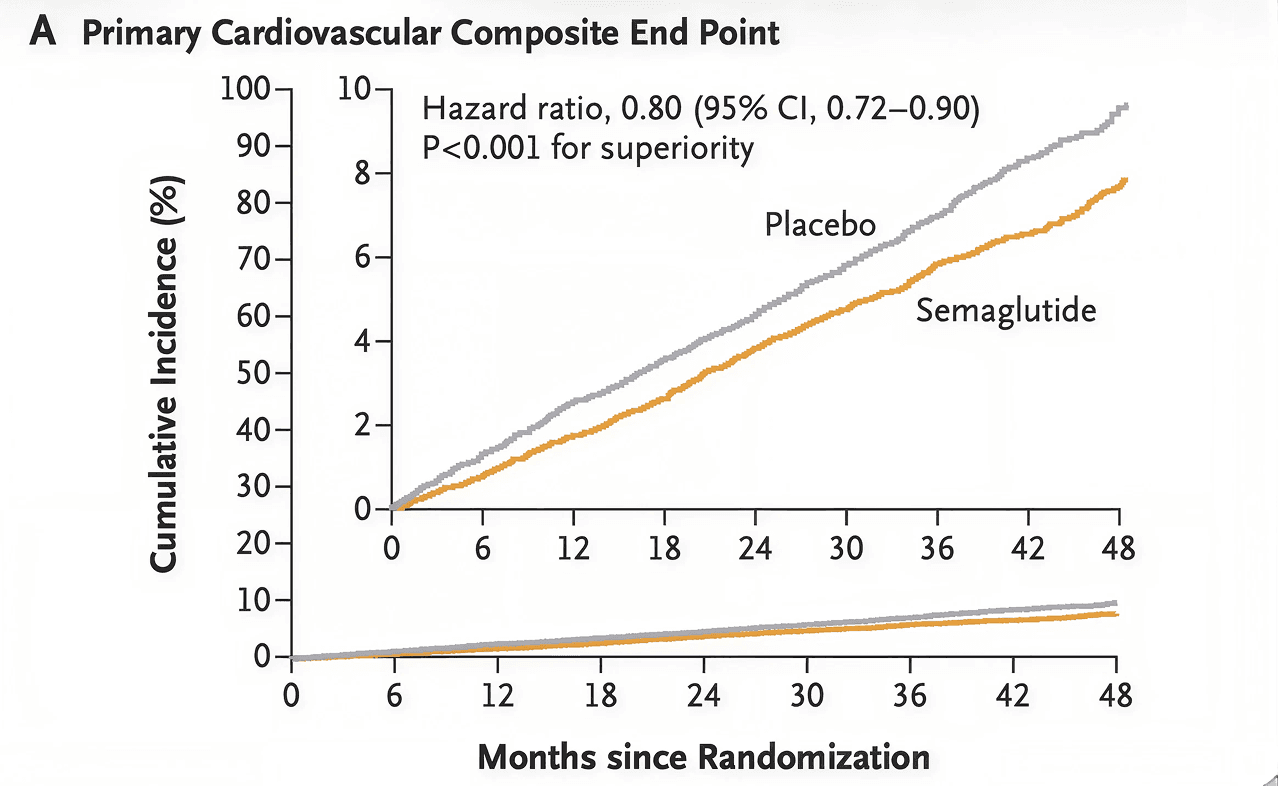
People with obesity, type 2 diabetes, insulin resistance, metabolic syndrome, or cardiovascular disease often benefit most from long term GLP-1 therapy. These are chronic conditions that require sustained treatment. Short term use may produce temporary improvements, but long term use provides lasting metabolic and cardiovascular protection.
People who have struggled with weight regain after previous diets or medications may also benefit. GLP-1 therapy helps regulate the biological drivers of hunger and weight set point, making maintenance more achievable. If you want to explore whether long term GLP-1 therapy is right for you, you can check your eligibility here.
FAQs
Is it safe to take GLP-1 medications for years?
Yes. Long term studies show that GLP-1 medications are safe for continued use. Cardiovascular and metabolic benefits persist, and serious side effects remain rare.
Do side effects get worse over time?
No. Most side effects, especially gastrointestinal symptoms, improve after the first few months. Long term use does not cause progressive worsening.
Does long term GLP-1 use increase cancer risk?
No. Extensive studies have not found increased cancer risk in people using GLP-1 medications for several years.
What happens if I stop taking GLP-1s after using them long term?
Most people regain weight and lose metabolic benefits after stopping. This reflects the chronic nature of obesity rather than medication failure.
How long have GLP-1 medications been studied?
Liraglutide has been used since 2010, providing over ten years of safety data. Semaglutide has been studied for over five years. Tirzepatide is newer but builds on similar mechanisms.
Check Your Eligibility
If you want to learn whether GLP-1 treatment could support your long term health and weight management goals, you can start by completing Mochi's eligibility questionnaire. It only takes a few minutes and helps our clinical team understand your goals and health history so they can provide personalized guidance. Check your eligibility here.
References:
Apovian, C. M., et al. (2023). Long-term weight loss with semaglutide: The STEP trials at 104 weeks. Obesity, 31(5), 1229–1241. https://doi.org/10.1002/oby.23742
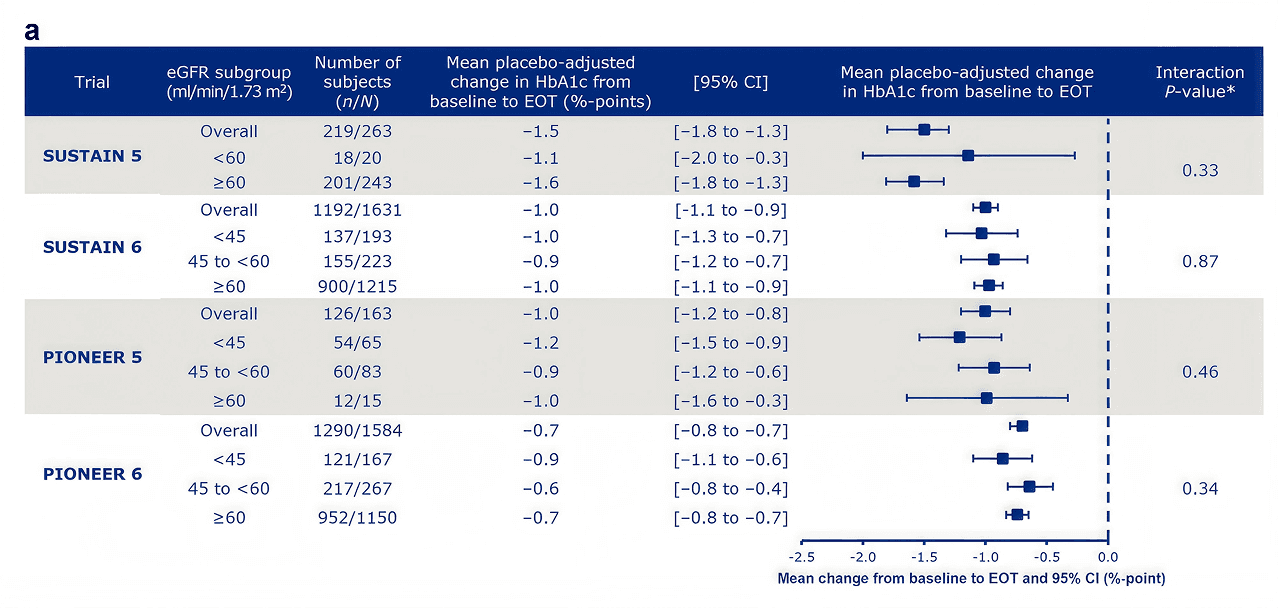
Cherney, D. Z. I., Hadjadj, S., Lawson, J., Mosenzon, O., Tuttle, K., Vrhnjak, B., Rasmussen, S., & Bain, S. C. (2021). Hemoglobin A1c reduction with the GLP-1 receptor agonist semaglutide is independent of baseline eGFR: Post hoc analysis of the SUSTAIN and PIONEER programs. Diabetes, Obesity and Metabolism, 23(12), 2842–2849. https://doi.org/10.1111/dom.14535
Lincoff, A. M., Brown-Frandsen, K., Colhoun, H. M., et al. (2023). Semaglutide and cardiovascular outcomes in obesity without diabetes. New England Journal of Medicine, 389(24), 2221–2232. https://doi.org/10.1056/NEJMoa2307563
Marso, S. P., Daniels, G. H., Brown-Frandsen, K., et al. (2016). Liraglutide and cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine, 375(4), 311–322. https://doi.org/10.1056/NEJMoa1603827
Marso, S. P., Bain, S. C., Consoli, A., et al. (2016). Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. New England Journal of Medicine, 375(19), 1834–1844. https://doi.org/10.1056/NEJMoa1607141
Perkovic, V., Tuttle, K. R., Rossing, P., et al. (2024). Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. New England Journal of Medicine, 390(2), 117–127. https://doi.org/10.1056/NEJMoa2403347
Rubino, D., Abrahamsson, N., Davies, M., et al. (2021). Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: The STEP 4 randomized clinical trial. JAMA, 325(14), 1414–1425. https://doi.org/10.1001/jama.2021.3224
Wilding, J. P. H., Batterham, R. L., Calanna, S., et al. (2021). Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine, 384(11), 989–1002. https://doi.org/10.1056/NEJMoa2032183
Zhong, V. W., Pfaff, E. R., Beavers, D. P., et al. (2022). Use of glucagon-like peptide-1 receptor agonists and risk of thyroid cancer: A meta-analysis. Diabetes Care, 45(12), 2920–2927. https://doi.org/10.2337/dc22-0826
Share this post
Weight loss
More articles
Read next






For iOS & Android






